Tirzepatide Dosage Guide: Protocols, Titration, and Research Data
Tirzepatide dosage guide searches usually come from one place: people want a clear answer on where dosing starts, how fast it increases, and what the research actually used. That sounds simple. It is not always simple in practice because clinical trial protocols, prescription labeling, and gray-market peptide products are not the same thing.
PeptidePick preferred picks
Use the highest-value vendor routes first.
Pinnacle is first for the 15% discount code. Ascension is the broad-catalog default when you want the cleaner research-only route.
Research-only affiliate links. Verify COAs, labels, and shipping terms before checkout.
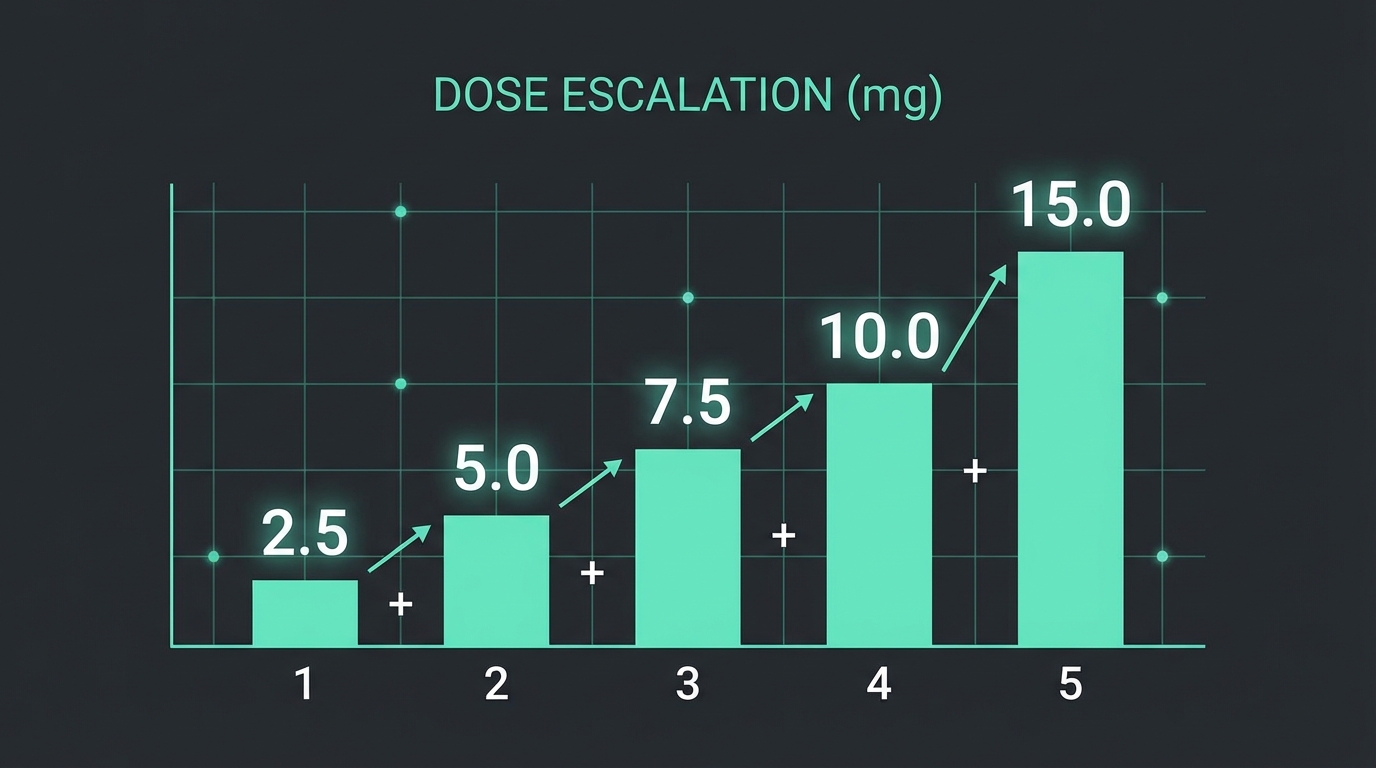
Here is the short version. Published tirzepatide trials used a low starting dose, then stepped up slowly in 2.5 mg increments every 4 weeks to improve tolerability. Most problems show up during escalation, not after a stable maintenance dose is reached.
TL;DR
- Tirzepatide trials typically started at 2.5 mg once weekly.
- Dose increases were usually 2.5 mg every 4 weeks.
- Common maintenance targets in research were 5 mg, 10 mg, and 15 mg weekly.
- Nausea and diarrhea were the most common adverse effects, especially during dose escalation.
- Research-use tirzepatide is not the same thing as an FDA-approved prescription product.
How tirzepatide dosing works
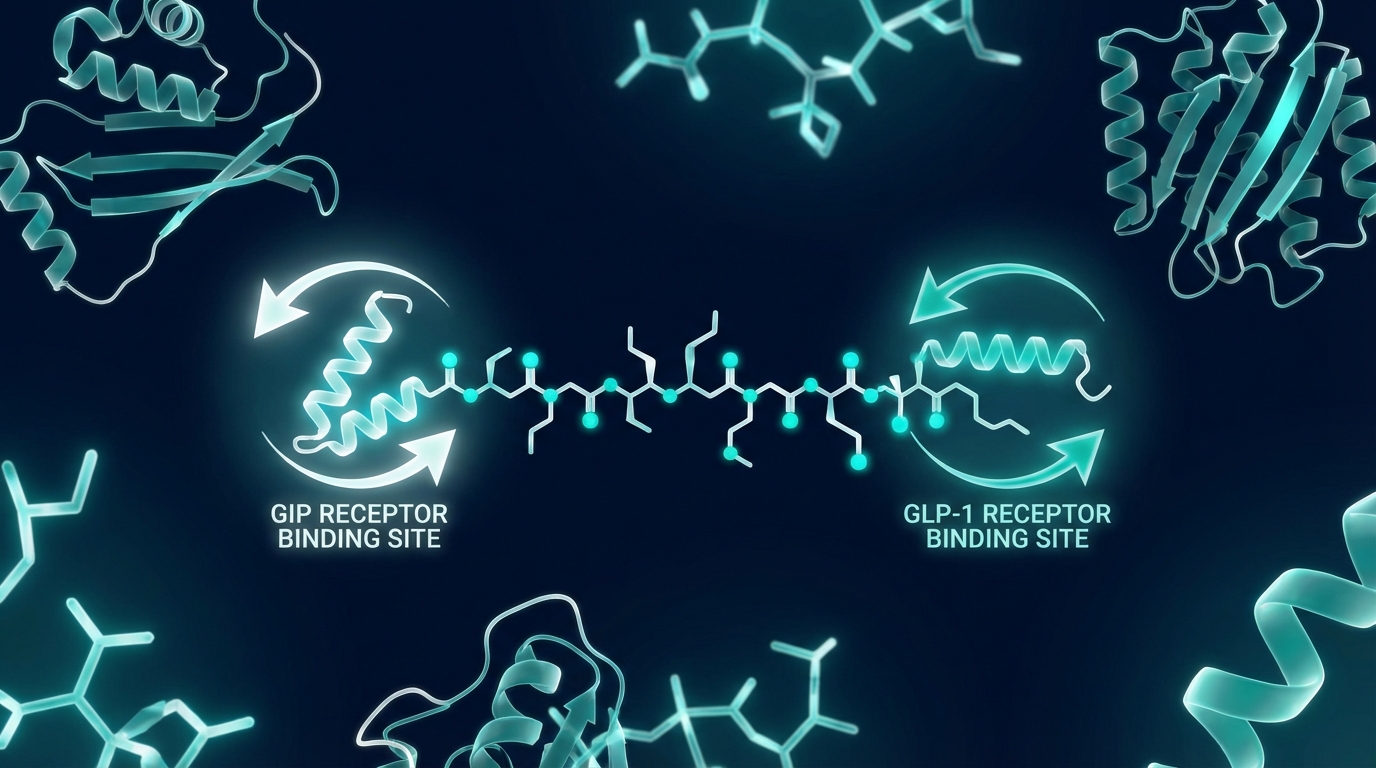
Tirzepatide is a dual GIP and GLP-1 receptor agonist. That dual action is a big reason it gets so much attention in weight-loss and glycemic-control discussions. It also helps explain why dose escalation matters so much.
A low starting dose is not meant to be the final effective dose for most protocols. It is mainly there to help people tolerate the gastrointestinal effects that tend to appear early. Based on the published trial designs, the smartest takeaway is not "go higher fast." It is "start low and let the body adapt."
If you are comparing GLP-focused compounds, this fits with what we covered in tirzepatide vs semaglutide and in our broader guide to peptides for weight loss.
Looking for a GLP-focused tirzepatide source to research?
Apollo Peptide Sciences specializes in GLP-1 research peptides and growth factors, which makes it a natural first stop for this category.
Shop Apollo GLP-1 Research Catalog →
Specializing in GLP-1 research peptides and growth factors
Trial-based tirzepatide dosage guide and titration schedule
The cleanest research reference point comes from SURMOUNT-1 and SURPASS-5. In both settings, tirzepatide was initiated at 2.5 mg once weekly. Then the dose was increased by 2.5 mg every 4 weeks until the assigned maintenance dose was reached.
That means the common trial ladder looked like this:
| Weeks | Weekly dose | Purpose |
|---|---|---|
| 1-4 | 2.5 mg | Adaptation and tolerability |
| 5-8 | 5 mg | First full therapeutic step used in trials |
| 9-12 | 7.5 mg | Bridge dose for escalation |
| 13-16 | 10 mg | Common maintenance target |
| 17-20 | 12.5 mg | Bridge dose for escalation |
| 21+ | 15 mg | Highest common maintenance dose in major trials |
That schedule is why many "tirzepatide dosage guide" pages feel repetitive. The base ladder really is straightforward. But what often gets skipped is the reason for the spacing. Four-week jumps were used because side effects cluster during escalation, and slower increases tend to be easier to tolerate.
SURMOUNT-1 ran for 72 weeks in adults with obesity and reported mean weight reductions of 15.0% at 5 mg, 19.5% at 10 mg, and 20.9% at 15 mg versus 3.1% with placebo. That does not mean everyone needs 15 mg. It means higher maintenance doses produced larger average weight changes in that study population.
For readers who are also trying to understand peptide math, our free peptide reconstitution calculator and guide on how to reconstitute peptides are the two references you should keep open.
Side effects by dose
The biggest reason tirzepatide protocols move slowly is side effects. In SURPASS-5, the most common treatment-emergent adverse events were diarrhea and nausea. Diarrhea occurred in 12% to 21% of tirzepatide groups versus 10% with placebo. Nausea occurred in 13% to 18% versus 3% with placebo.
SURMOUNT-1 described gastrointestinal adverse events as the most common issues, mostly mild to moderate, and occurring primarily during dose escalation. That is the part a lot of competitor articles flatten into one sentence. The timing matters. If symptoms flare during a recent jump, that context changes how the protocol should be interpreted.
- Lower doses usually improve tolerability. That is why 2.5 mg is a starting step, not a full-effect target.
- Escalation brings more friction. Nausea, diarrhea, reduced appetite, and fullness are most common during the climb.
- Discontinuation rises with dose in some trials. SURPASS-5 showed discontinuation at 10% for 5 mg, 12% for 10 mg, 18% for 15 mg, versus 3% for placebo.
That does not prove 15 mg is a bad dose. It shows the tradeoff is real. More effect can come with more dropout pressure. Some readers want a neat answer here, but there really is a judgment call between pushing for maximal effect and protecting tolerability.
Want the broadest catalog of tirzepatide-adjacent research options?
Limitless carries 118+ research peptides in injectable, spray, and capsule forms. Start with the free VIP signup link so your referral tracking sticks before checkout.
Unlock Limitless VIP Catalog →
118+ research peptides in injectable, spray, and capsule forms - create a free account to access full catalog
Use code PeptidePick for a discount at checkout
Research-use tirzepatide vs prescription products
This is where the article needs to stay honest. Prescription tirzepatide products are regulated drugs approved for specific uses. Research-use tirzepatide sold by peptide vendors is a different category. You should not blur those together.
If you are buying from a research vendor, the key questions are purity data, batch testing, storage, and whether the vendor is transparent about intended use. Legal status also matters. Our breakdown of are peptides legal is worth reading before you buy anything.
And if you are still comparing suppliers, this guide to the best peptide companies helps narrow the field without guessing from forum posts.
One more practical note. If the product arrives lyophilized, dosing accuracy depends on proper mixing, syringe math, and injection method. That is why the calculator and reconstitution guides above are not side resources. They are part of safe protocol planning.
Practical tirzepatide dosage questions people ask
What is the normal starting dose?
In the major tirzepatide trials, the standard starting point was 2.5 mg once weekly. That was used as a tolerability step before escalation.
How long should someone stay at each dose?
Research protocols commonly used 4 weeks at each step before increasing by another 2.5 mg. Faster changes may look tempting on paper, but they move away from what the published data actually tested.
Is 15 mg always better than 5 mg?
Not automatically. Higher doses produced larger average weight reductions in SURMOUNT-1, but they also come with more tolerability pressure. For some people, the best dose is the highest dose they can actually stay on without quitting.
What if someone misses a weekly dose?
That question usually belongs to product-specific labeling or clinician guidance, not peptide message boards. For research buyers, the key point is consistency matters, and ad hoc catch-up dosing is a bad place to improvise.
Does tirzepatide need reconstitution?
Prescription pens do not. Many research-use peptide products do. If that is your situation, read our guides on how to mix peptides and SubQ vs intramuscular injection for peptides before touching the vial.
How to source and handle tirzepatide research products
For weight and GLP-focused articles, vendor fit matters. Apollo makes sense because it leans into GLP-1 research peptides. Limitless makes sense because it has a huge catalog and the VIP signup path locks in tracking before checkout. Pinnacle belongs in the mix because it carries GLP-1SG, GLP-2TZ, and GLP-3RT alongside other research peptides, and the brand-specific discount is real.
If you want a starting shortlist, these are also the kinds of vendors that show up in our coverage of the best peptides for weight loss and adjacent comparison pieces like retatrutide vs semaglutide.
Before buying, check these basics:
- Is there third-party testing or at least a clear purity claim?
- Does the site clearly separate research products from prescription medicine claims?
- Do you understand storage, mixing, and weekly dose calculations before ordering?
- Are you buying based on trial data, or just chasing the highest number on social media?
That last one sounds blunt, but it matters. Most dosing mistakes happen when enthusiasm outruns protocol discipline.
Need another proven vendor with a peptide-specific discount?
Pinnacle Peptide Labs stocks multiple GLP research options and makes the value case stronger with a standing PeptidePick discount code.
99% pure research peptides - use code Peptidepick15 for 15% off
Use code Peptidepick15 for 15% off your order

FAQ
What dose of tirzepatide do trials usually start with?
Major trials such as SURMOUNT-1 and SURPASS-5 started tirzepatide at 2.5 mg once weekly.
How often do tirzepatide doses increase in research protocols?
The common protocol was an increase of 2.5 mg every 4 weeks until the target maintenance dose was reached.
What maintenance doses have been studied most?
Large phase 3 studies commonly evaluated 5 mg, 10 mg, and 15 mg once weekly.
Which side effects are most common during tirzepatide escalation?
Nausea and diarrhea were among the most common adverse events reported in published trials, with GI effects most noticeable during dose escalation.
Is research tirzepatide the same as a prescription tirzepatide pen?
No. Prescription tirzepatide products are regulated drugs. Research-use tirzepatide sold online is a separate category and should not be treated as interchangeable.
Where can I compare vendors before buying?
Start with our guide to the best peptide companies, then compare catalog fit, testing transparency, and storage requirements.
Related articles
- Tirzepatide vs Semaglutide
- Peptides for Weight Loss
- Best Peptides for Weight Loss
- How to Reconstitute Peptides
- Free Peptide Reconstitution Calculator
- Are Peptides Legal to Buy?
What competitor tirzepatide dosage guides usually miss
Most ranking pages cover the same basic ladder: 2.5 mg start, then move up every few weeks. That part is fine. The weak spot is that many of them stop right where the useful conversation should start.
They often leave out discontinuation data. That matters because a dosage guide should not just show what was assigned on paper. It should show what people were actually able to stay on through the end of a study.
They also blur prescription labeling with research-use peptide sourcing. That is risky. A person reading about FDA-approved tirzepatide pens is dealing with a very different quality-control environment than someone ordering a lyophilized vial from a peptide vendor.
Another thing that gets missed is the role of pacing. The four-week jumps used in major trials were not arbitrary. They gave participants time to adapt before the next increase. Social media shortcuts usually ignore that.
How to interpret trial data without overreading it
SURMOUNT-1 and SURPASS-5 are useful anchors, but they are still study environments. Participants were screened, monitored, and followed with far more structure than the average person has outside a trial.
So the right move is to treat those numbers as guardrails, not permission slips. If a protocol needed a 20-week escalation period in a controlled setting, that should make anyone pause before treating rapid jumps as normal.
And there is another nuance here. Weight-loss averages can make the highest dose look like the obvious winner, but averages hide dropouts, side effects, and the simple fact that some people do better on a dose they can sustain.
That is less exciting than a headline about maximal loss. It is also a lot closer to reality.
Storage, reconstitution, and dose math mistakes to avoid
Research tirzepatide buyers often spend most of their energy comparing milligram numbers and not enough energy on handling. But bad mixing math can ruin a protocol before the first weekly dose is even drawn.
If the vial is lyophilized, the final concentration depends on how much bacteriostatic water is added. That means the amount on the syringe is not meaningful until you know the full reconstitution math. This is exactly why the calculator exists.
Storage errors matter too. Heat, repeated agitation, and sloppy refrigeration can all create problems. Our article on how to reconstitute peptides covers the basics, and the companion guide to how to mix peptides helps with the practical steps.
So before anyone worries about 7.5 mg versus 10 mg, the first question should be simpler: do you trust the concentration in the syringe to match the plan on paper?