SubQ vs Intramuscular Injection for Peptides: Which Method Is Better?
Subcutaneous (SubQ) injection is the standard method for most research peptides. It is easier to perform, less painful, and provides steady absorption. Intramuscular (IM) injection offers faster absorption and may be preferred for localized delivery in certain protocols. For peptides like BPC-157, TB-500, and most growth hormone secretagogues, SubQ is the go-to choice for the majority of researchers.
Choosing between subcutaneous and intramuscular injection is one of the first decisions researchers face when working with peptides. Both methods deliver compounds effectively, but they differ in absorption speed, comfort, ease of use, and suitability for specific peptides.
This guide breaks down the key differences between SubQ and IM injection so you can select the right method for your research goals. If you are new to peptide preparation, start with our guide to reconstituting peptides before moving on to injection technique.
What Is Subcutaneous (SubQ) Injection?
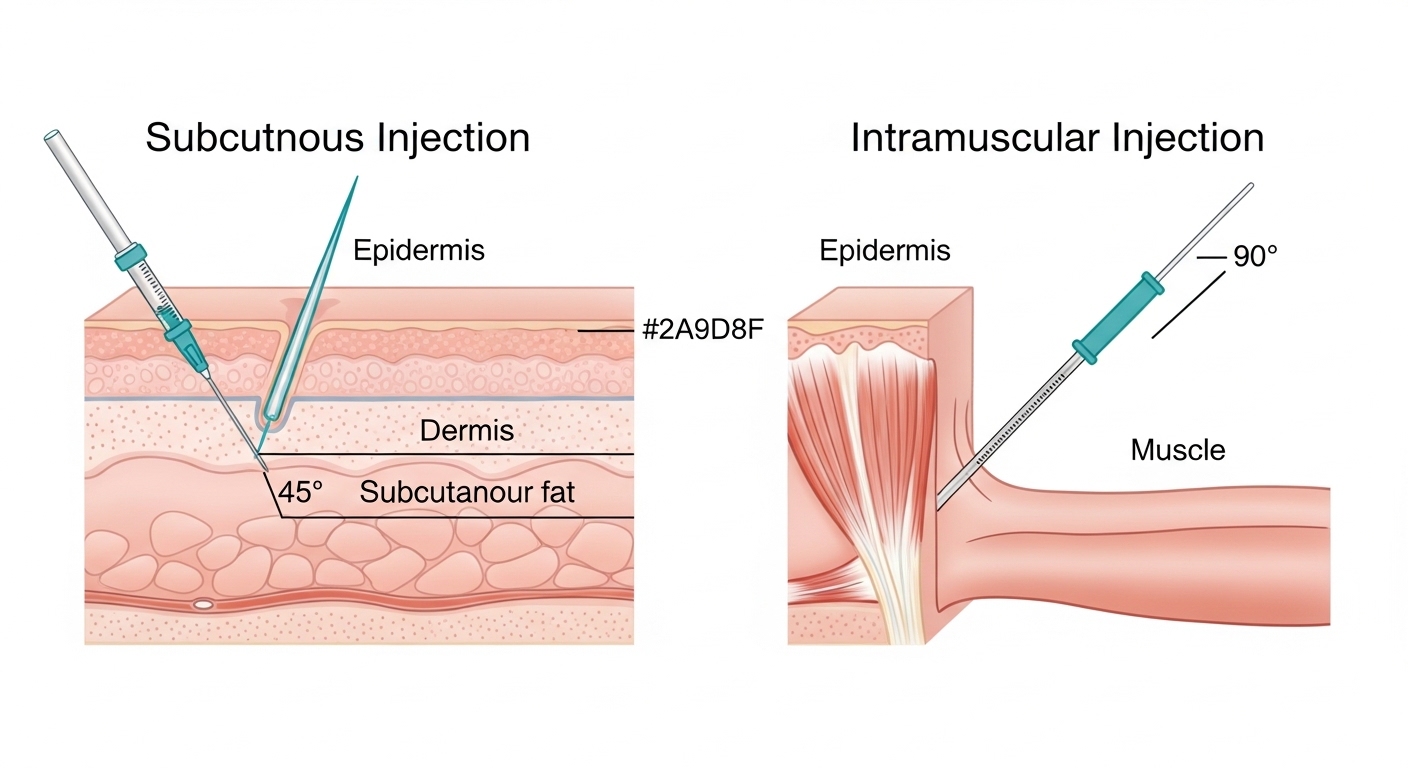
A subcutaneous injection delivers a compound into the fatty tissue layer just beneath the skin. This is the same method used for insulin injections and many pharmaceutical peptides. The needle enters at a 45 to 90 degree angle, depending on the amount of subcutaneous fat at the injection site, and typically reaches a depth of only 4 to 6 millimeters.
SubQ injection is the most common method in peptide research for good reason. It requires minimal technique, uses small and comfortable needles, and provides reliable absorption for the vast majority of peptides.
What Is Intramuscular (IM) Injection?
An intramuscular injection delivers a compound directly into muscle tissue. Because muscles have a rich blood supply, IM injections generally result in faster absorption compared to SubQ. The needle enters at a 90 degree angle and penetrates through the skin and subcutaneous fat layer into the underlying muscle, typically reaching a depth of 25 to 38 millimeters.
IM injections are standard for certain medications like testosterone and some vaccines. In peptide research, IM is less commonly used but has specific applications where faster uptake or localized delivery matters.
SubQ vs Intramuscular Injection: Side-by-Side Comparison
| Factor | Subcutaneous (SubQ) | Intramuscular (IM) |
|---|---|---|
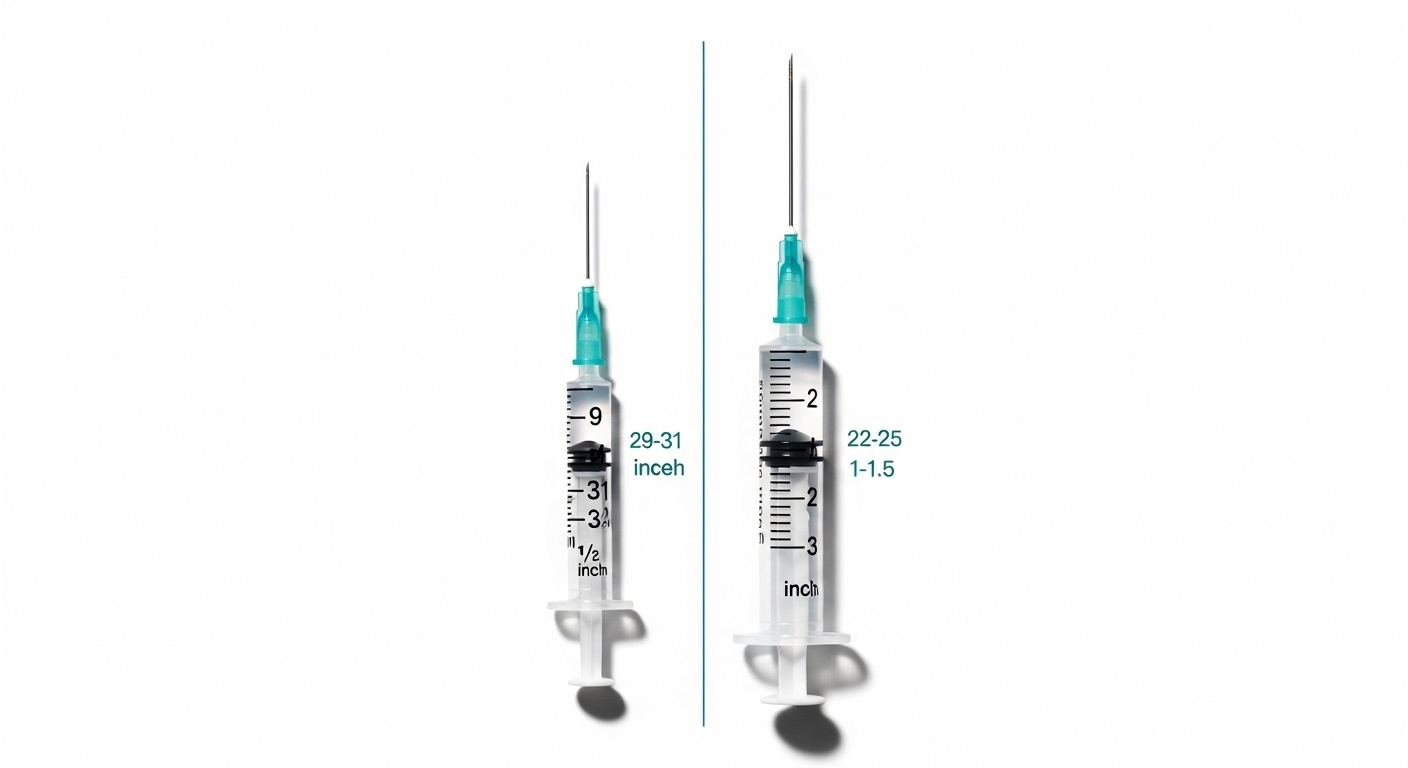
| Needle Gauge | 29-31 gauge (thin) | 22-25 gauge (thicker) |
| Needle Length | 0.5 inch (12.7mm) | 1 – 1.5 inch (25-38mm) |
| Injection Depth | Fat layer (4-6mm) | Muscle tissue (25-38mm) |
| Absorption Rate | Moderate, steady release | Faster peak absorption |
| Pain Level | Minimal | Mild to moderate |
| Ease of Use | Very easy (beginner-friendly) | Moderate (requires technique) |
| Injection Volume | Up to 1-2 mL | Up to 3-5 mL (depending on site) |
| Best For | Most peptides, daily protocols | Localized delivery, larger volumes |
Absorption Rate Differences
The primary functional difference between SubQ and IM injection comes down to how quickly the body absorbs the compound.
Muscle tissue has a denser network of blood vessels compared to subcutaneous fat. This means IM injections typically reach peak blood concentration faster. Research on insulin and growth hormone analogs consistently shows that IM injection produces a sharper, earlier peak, while SubQ injection creates a more gradual, sustained release curve.
For most peptide research applications, the slower and steadier SubQ absorption profile is actually preferable. Peptides like growth hormone releasing peptides (GHRPs) and growth hormone secretagogues benefit from a sustained presence rather than a sharp spike. The extended absorption window from SubQ injection more closely mimics natural pulsatile release patterns.
However, there are cases where faster absorption through IM injection may be relevant. Researchers working with compounds that require rapid systemic availability, or those targeting specific muscle groups for localized effects, may find IM delivery more appropriate.
Which Peptides Work Better With Which Method
Peptides Best Suited for SubQ Injection
The majority of research peptides are administered subcutaneously. This includes:
- BPC-157 – Commonly injected SubQ near the area of interest. For gut-related research, SubQ abdominal injection is standard. For joint or tendon research, injecting SubQ as close to the target area as possible is the most common protocol.
- TB-500 (Thymosin Beta-4) – Works systemically regardless of injection site. SubQ in the abdomen is the standard approach since TB-500 acts throughout the body rather than locally.
- CJC-1295 / Ipamorelin – SubQ abdominal injection is standard for these growth hormone secretagogues.
- PT-141 – SubQ injection in the abdomen or thigh.
Peptides That May Benefit From IM Injection
Fewer peptides call for IM injection, but there are scenarios where it makes sense:
- BPC-157 for deep muscle injuries – Some researchers prefer IM injection directly into the affected muscle when studying deep tissue repair.
- BPC-157 + TB-500 stacks – In protocols targeting specific muscle groups, IM injection at the injury site is sometimes preferred for the BPC-157 component while TB-500 is injected SubQ elsewhere.
- IGF-1 LR3 – Often administered IM into the target muscle group in bodybuilding research contexts.
Common Injection Sites
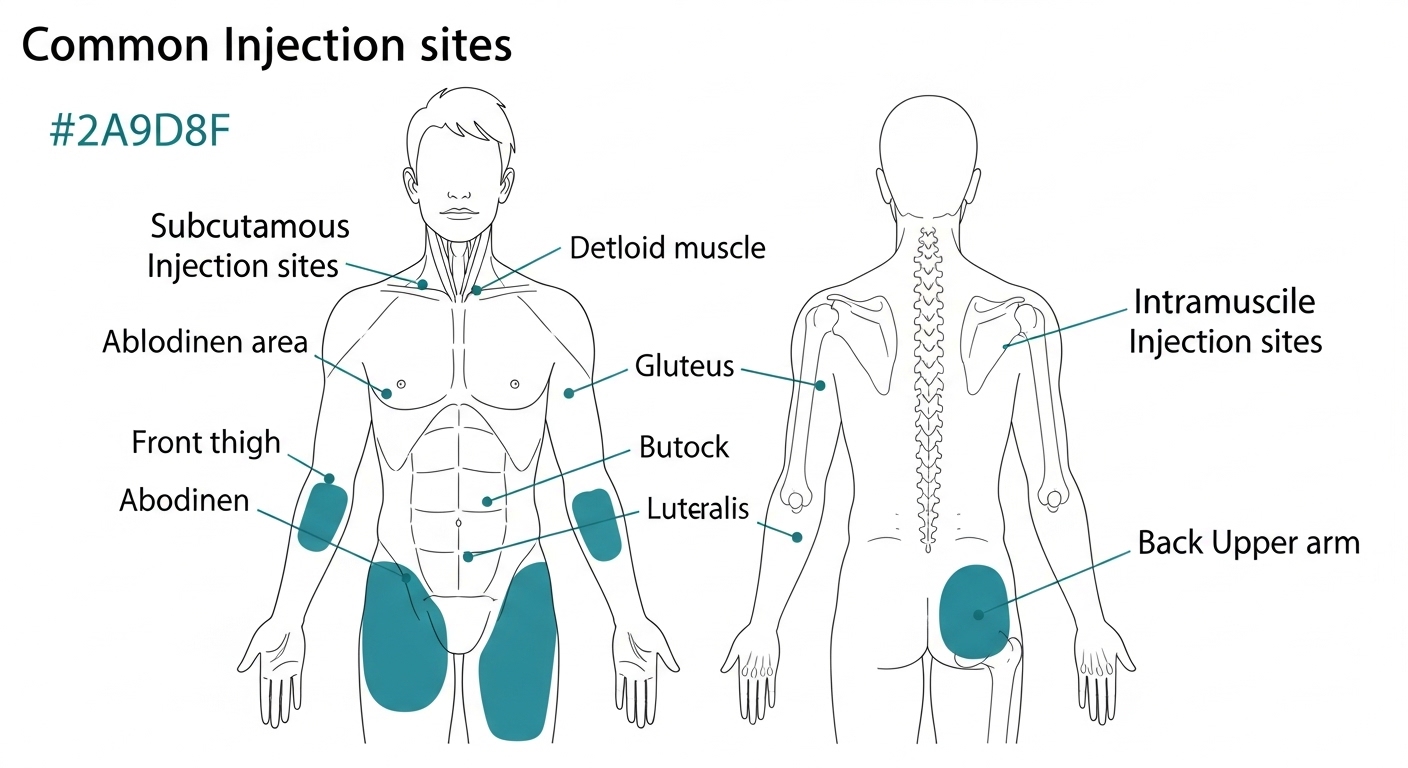
SubQ Injection Sites
- Abdomen (most common) – Pinch the skin 2 inches from the navel. Avoid the area directly around the belly button. Rotate between left and right sides.
- Upper thigh – Front or outer thigh, midway between knee and hip. Easy to reach and relatively painless.
- Back of the upper arm – The tricep area has accessible subcutaneous tissue, though it can be harder to reach solo.
- Love handle area – The flanks offer ample subcutaneous fat for comfortable injections.
IM Injection Sites
- Deltoid (shoulder) – Good for smaller volumes (up to 1 mL). Locate the thickest part of the deltoid muscle, roughly two finger-widths below the acromion.
- Vastus lateralis (outer thigh) – The easiest IM site for self-injection. Target the outer middle third of the thigh.
- Ventrogluteal (hip) – Preferred for larger volumes. Harder to reach for self-administration but has fewer nerves and blood vessels.
Needle Gauge and Length Recommendations
Choosing the right needle makes a significant difference in comfort and accuracy.
For SubQ Injections
- Gauge: 29-31 gauge (higher number = thinner needle)
- Length: 0.5 inch (12.7mm) or 5/16 inch (8mm) for insulin syringes
- Syringe type: Standard insulin syringes (0.5 mL or 1 mL) work perfectly
For IM Injections
- Gauge: 23-25 gauge
- Length: 1 inch for deltoid and thigh, 1.5 inch for ventrogluteal
- Syringe type: Standard luer-lock syringes (1-3 mL)
Many researchers use a two-needle technique for IM injections: draw with an 18-20 gauge needle, then swap to a 25 gauge needle for injection. This keeps the injection needle sharp since drawing through rubber stoppers can dull the tip.
Quick Step-by-Step for Each Method
For full detailed instructions with photos, see our complete how to inject peptides guide. Here is a brief overview of each method.
SubQ Quick Steps
- Clean the injection site with an alcohol swab and let it dry.
- Pinch a fold of skin between your thumb and forefinger.
- Insert the needle at a 45 to 90 degree angle (90 degrees for insulin syringes with short needles).
- Inject slowly and steadily.
- Release the skin pinch, withdraw the needle, and apply gentle pressure with a cotton ball.
IM Quick Steps
- Clean the injection site with an alcohol swab and let it dry.
- Stretch the skin taut with your non-dominant hand.
- Insert the needle at a 90 degree angle in one smooth motion.
- Note: aspiration (pulling back the plunger to check for blood) is no longer recommended by the CDC for standard IM injection sites like the deltoid and vastus lateralis.
- Inject slowly. Withdraw and apply pressure.
Pain Comparison and Tips to Minimize Discomfort
SubQ injections are generally less painful than IM injections. The thinner needles used for SubQ (29-31 gauge) cause less tissue disruption, and the subcutaneous fat layer has fewer pain receptors than muscle tissue.
That said, both methods are manageable. Here are practical tips to reduce discomfort:
- Let alcohol dry completely before inserting the needle. Injecting through wet alcohol stings.
- Use a fresh needle every time. Reused needles become dull and cause more pain.
- Inject at room temperature. Cold peptide solutions can cause more discomfort. Let the vial warm up for 10-15 minutes before injecting.
- Inject slowly. Rapid injection increases pressure in the tissue and causes more pain.
- Rotate injection sites. Repeated injections in the same spot cause scar tissue buildup, making future injections more painful.
- Relax the muscle (for IM). Tensing up increases pain significantly. Sit or lie in a position where the target muscle is fully relaxed.
- Ice the area for 30 seconds beforehand if you are sensitive to needle insertion.
When to Choose SubQ vs IM Based on Research Goals
Choose SubQ when:
- Using peptides that work systemically (TB-500, CJC-1295, Ipamorelin, most others)
- Running daily injection protocols where comfort and simplicity matter
- Working with standard peptide doses under 1 mL
- You are new to peptide research and want the easiest method
- Targeting general healing or recovery rather than a specific muscle
Choose IM when:
- Your protocol specifically requires intramuscular delivery
- Targeting a specific muscle group for localized research (deep tissue BPC-157 protocols)
- Working with compounds known to have better IM bioavailability
- Injecting larger volumes that would be uncomfortable SubQ
- Faster absorption timing is important to your protocol
Common Mistakes to Avoid
- Using the wrong needle length for IM. A needle that is too short may deposit the compound in subcutaneous tissue rather than muscle, leading to inconsistent results. Match needle length to the injection site and your body composition.
- Injecting too fast. Both SubQ and IM injections should be performed slowly. Rapid injection causes unnecessary pain, bruising, and inconsistent absorption.
- Not rotating injection sites. Using the same spot repeatedly leads to lipohypertrophy (tissue hardening) for SubQ and scar tissue for IM. Rotate between at least 4-6 sites.
- Skipping the alcohol swab. Infection risk is low but not zero. Clean the site every time. It takes five seconds.
- Reusing needles. Single-use needles are inexpensive. A fresh, sharp needle reduces pain, prevents infection, and ensures accurate delivery.
- Choosing IM when SubQ would work fine. Unless your research protocol specifically calls for IM, there is usually no advantage to the deeper, more painful injection. SubQ is the default for a reason.
- Injecting into bruised or irritated tissue. Wait for the site to heal fully before using it again.
Where to Source Quality Research Peptides
Injection method only matters if your peptides are pure and properly manufactured. We have tested and reviewed dozens of vendors. Here are three that consistently deliver third-party tested, high-purity peptides:
- Swiss Chems – Wide peptide selection with published COAs for every batch.
- Core Peptides – Competitive pricing and fast shipping on popular compounds.
- Paradigm Peptides – US-based with rigorous third-party testing and excellent customer support.
See our full best peptide companies ranking for detailed reviews of each vendor.
Related Articles
- How to Inject Peptides: Complete Step-by-Step Guide
- How to Reconstitute Peptides (With Calculator)
- BPC-157 Guide: Benefits, Dosing, and Research
- TB-500 Guide: What Researchers Need to Know
- The Wolverine Stack: BPC-157 + TB-500 Protocol
- Best Peptide Companies: Ranked and Reviewed
Ready to Start Your Peptide Research?
Find trusted, third-party tested peptide vendors in our comprehensive comparison guide.
Frequently Asked Questions
Is SubQ or IM better for BPC-157?
SubQ is the standard for most BPC-157 research protocols. Inject SubQ near the area of interest for best results. IM may be considered only for deep muscle injuries where the target tissue sits well beneath the subcutaneous layer.
Do SubQ injections absorb slower than IM?
Yes, SubQ injections generally absorb more slowly than IM, producing a more gradual and sustained release. For most peptides, this slower absorption profile is actually desirable and more closely mimics natural physiological patterns.
Can I use insulin syringes for peptide injections?
Yes. Insulin syringes (typically 29-31 gauge, 0.5 inch) are ideal for SubQ peptide injections. They are inexpensive, widely available, and perfectly sized for standard peptide doses. See our injection guide for detailed syringe recommendations.
Does injection site matter for TB-500?
TB-500 is a systemic peptide, meaning it circulates throughout the body regardless of where you inject it. SubQ injection in the abdomen is the most common and convenient approach. There is no need to inject near an injury site with TB-500.
How do I know if I injected SubQ or IM by accident?
If you used a short insulin needle (0.5 inch or less) and pinched the skin, you almost certainly injected SubQ. Accidentally hitting muscle with a short needle is unlikely in areas with adequate subcutaneous fat like the abdomen. If you intended IM and used a longer needle without pinching, the injection likely reached muscle tissue.
What gauge needle hurts the least?
Higher gauge numbers mean thinner needles and less pain. A 30 or 31 gauge needle (used for SubQ) is barely noticeable for most people. For IM injections, a 25 gauge needle is the best balance between comfort and practicality.