Vendor shortcuts
Compare the right source before you keep reading
Pick the lane that matches your research goal, then verify current COAs, label language, and shipping policy on the vendor page.
Research-only affiliate links. PeptidePick may earn a commission at no extra cost to you.
Retatrutide Dosage Protocol: Titration, Timing, and Research Guidelines
Meta description: Retatrutide dosage protocol explained with trial titration schedules, timing, safety signals, reconstitution basics, and research-focused sourcing notes.
TLDR
The most cited retatrutide dosage protocol comes from Eli Lilly's phase 2 obesity trial, where once-weekly dosing was escalated gradually to improve tolerability. Trial arms included maintenance doses up to 12 mg, and gastrointestinal side effects rose as dose increased.
But there is no FDA-approved retatrutide dosing schedule yet. Any discussion of titration, timing, or reconstitution has to stay anchored to published trial methods rather than personal-use instructions.

What is retatrutide?
Retatrutide is a triple-agonist peptide studied for obesity and metabolic disease. It targets GLP-1, GIP, and glucagon receptors, which makes it broader than semaglutide and tirzepatide from a receptor standpoint.
The headline data most people cite comes from the 2023 phase 2 obesity trial published in the New England Journal of Medicine. That study reported substantial weight reduction at 24 and 48 weeks, with stronger effects at higher maintenance doses. It also confirmed a familiar pattern in the GLP-1 category: more efficacy often comes with more gastrointestinal friction.
So the first thing to understand is simple. There is no approved market label with a finalized retatrutide dose. The closest thing to a usable protocol is the titration structure tested in controlled trials.
Looking for GLP research peptides from a weight-loss focused vendor?
Apollo Peptide Sciences centers its catalog around GLP compounds and growth-factor research products, which makes it a natural first stop for this category.
Shop Apollo Peptide Sciences →
Specializing in GLP-1 research peptides and growth factors
Retatrutide dosage protocol used in trials
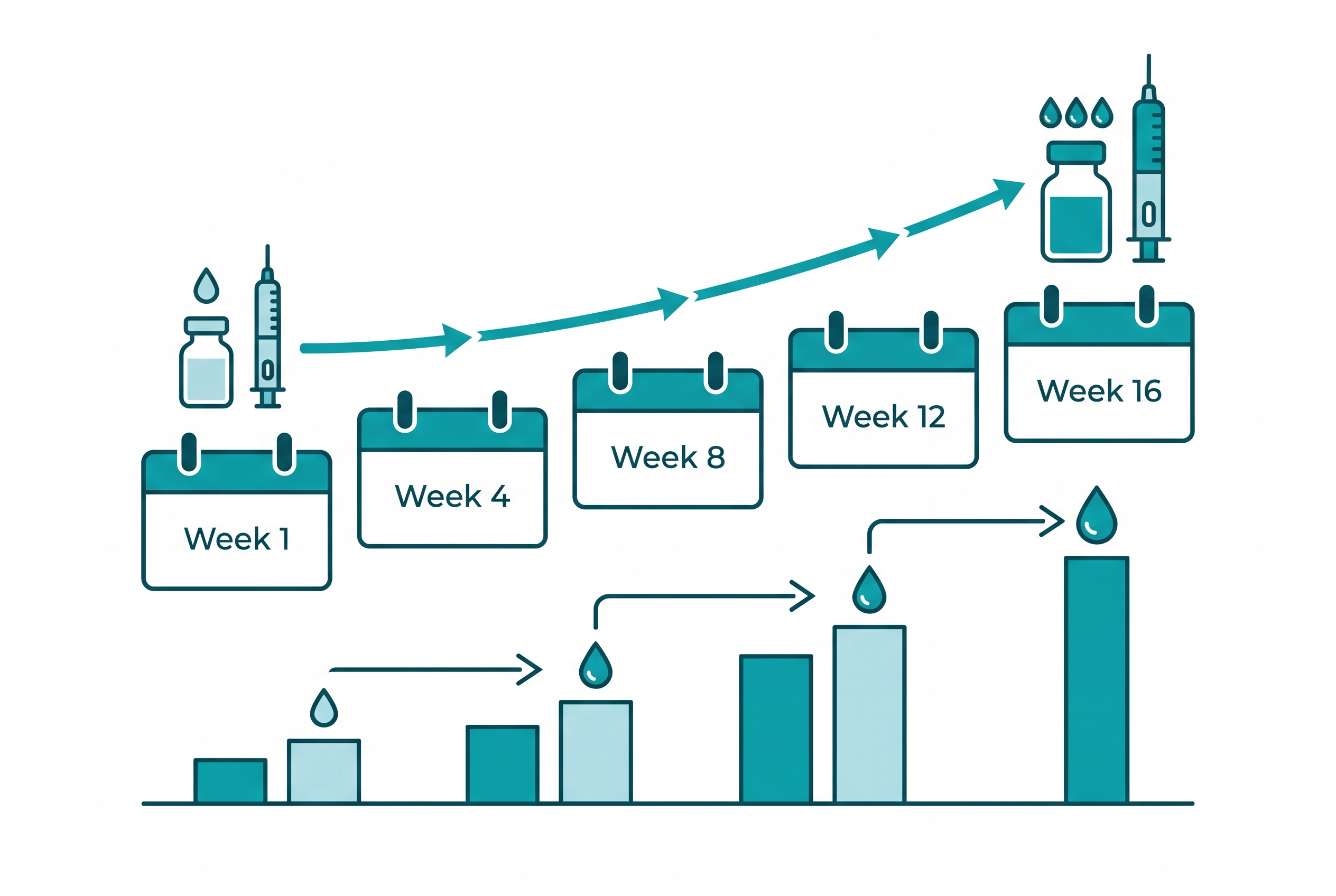
The phase 2 obesity trial is the main anchor for any serious discussion of a retatrutide dosage protocol. Public summaries of the study describe once-weekly dosing with step-up escalation, and published analyses reference maintenance groups at 1 mg, 4 mg, 8 mg, and 12 mg.
The key point is simpler. The trial design used gradual escalation to reach higher target doses while trying to limit nausea, vomiting, diarrhea, and treatment discontinuation.
| Trial element | What published sources indicate |
|---|---|
| Administration | Once-weekly injection in phase 2 obesity research |
| Maintenance doses studied | Arms included 1 mg, 4 mg, 8 mg, and 12 mg |
| Escalation strategy | Gradual titration over time rather than immediate high-dose exposure |
| Why escalation matters | GI tolerability became a bigger issue as dose increased |
| Status | Investigational only - no FDA-approved label dose |
Some follow-up liver-disease research also described dose escalations every 4 weeks. That does not prove one universal standard. Still, it supports the broader pattern: retatrutide has been studied with paced titration, not aggressive front-loading.
If you want a clearer baseline for dosing math, compare this article with our tirzepatide dosage guide and semaglutide guide. The drug class logic overlaps, even though the receptor profile does not.
Timing, titration, and why escalation matters
Weekly timing matters for two reasons. First, retatrutide was studied as a once-weekly injection. Second, slower step-ups give adverse effects time to declare themselves before the next jump.
The biggest issue readers miss is that tolerance is not just about comfort. In incretin-style trials, GI symptoms often drive dropouts. A protocol that looks efficient on paper can fall apart if subjects cannot stay on it long enough to reach the target arm.
- Nausea and vomiting were dose-related concerns in trial reporting.
- Diarrhea and appetite suppression may intensify after escalation steps.
- Heart-rate effects have also been discussed in trial commentary and deserve monitoring in formal research settings.
- No approved self-use schedule exists, which is why published trial methods matter more than forum guesses.
And this is where nuance matters. Higher-dose retatrutide arms produced the most impressive weight-loss numbers, but the best-looking endpoint is not automatically the best starting framework for every protocol discussion.
Want the broadest menu of research delivery formats?
Limitless Biotech stands out for injectable, spray, and capsule options across a huge catalog. Start with the VIP signup so the affiliate tracking cookie is set first.
Create your free Limitless Biotech account →
118+ research peptides in injectable, spray, and capsule forms - create a free account to view the full catalog
Use code PeptidePick for a discount at checkout
Reconstitution math and handling basics
Search intent around retatrutide dosage often spills into reconstitution math. That makes sense. People usually are not just asking about milligrams. They are trying to convert vial strength into syringe units.
But reconstitution is not specific to retatrutide. It is a general peptide handling skill. If you need the math framework, use the free peptide reconstitution calculator and review how to reconstitute peptides before touching any protocol worksheet.
For a deeper overview, our bacteriostatic water guide explains dilution basics, and how to mix peptides walks through the process step by step. Those pages matter because dosage errors often start as mixing errors.
One caveat is worth stating plainly. A vial concentration can make unit math look easy while still leaving the protocol itself unresolved. Clean arithmetic does not turn an investigational compound into an approved regimen.
What the evidence actually says about the retatrutide dosage protocol
Most SERP pages for this keyword chase a shortcut. They copy a dose ladder from discussion boards, add a few generic safety lines, and present it as if the matter is settled. It is not settled.
The best-supported points come from formal trial reporting and regulator-facing drug-class context. Those source types do not answer every practical question, but they do separate known information from recycled speculation.
- Phase 2 obesity data: the 2023 NEJM paper on retatrutide reported dose-dependent weight reduction over 24 and 48 weeks in adults with obesity.
- Maintenance arms: public summaries reference 1 mg, 4 mg, 8 mg, and 12 mg maintenance groups.
- Titration logic: escalation was gradual. The point was tolerability, especially around nausea, vomiting, and diarrhea.
- MASLD phase 2a reporting: later trial reporting also referenced dose increases every 4 weeks where applicable.
- Regulatory status: retatrutide is still investigational, which means no approved package insert defines a public dosing label.
- Class comparison: semaglutide and tirzepatide can rely on approved label schedules. Retatrutide cannot yet.
That gap matters because searchers often want a clean answer. The honest answer is messier. There is a trial-based framework, but there is still no approved retatrutide dose card to point at.
What competing pages usually miss
Competitor coverage around retatrutide dosage tends to break in the same few places. First, many pages collapse "trial dose" and "recommended dose" into one idea. Second, they skip the reason titration exists in the first place. Third, they rarely connect dosing with reconstitution math and sourcing quality on the same page.
A better article needs to answer all three. It should explain the trial structure, show why escalation exists, and route readers to the handling guides that prevent basic math errors.
It also helps to make one distinction explicit. Research protocols are not the same as medical treatment instructions. That sounds obvious, but a lot of ranking pages blur it.
Questions readers ask before they trust a dose chart
Search results and forum chatter around this topic usually circle the same themes:
- Is retatrutide dosed weekly or more often?
- What starting level was used before the 8 mg or 12 mg arms?
- How long should each escalation phase last?
- Does reconstitution change the target dose or just the syringe math?
- Why do some people compare it to semaglutide while others compare it to tirzepatide?
- Is there any approved prescription version yet?
Those questions are reasonable. But they also show why this keyword is tricky. Part of the audience wants research precision. Another part wants a personal-use answer that no responsible article can claim to provide.
So the safest path is to keep the page anchored to trial design, public study summaries, and clean handling references such as the calculator, mixing guide, and storage articles.
Retatrutide dosage protocol vs semaglutide and tirzepatide
Retatrutide gets compared with semaglutide and tirzepatide because all three sit in the metabolic-weight-loss conversation. But the dosing context is very different.
| Compound | Regulatory status | Dosing confidence level | Key point |
|---|---|---|---|
| Semaglutide | FDA-approved products exist | High | Label-based escalation schedules are public |
| Tirzepatide | FDA-approved products exist | High | Clinical and labeled titration structures are established |
| Retatrutide | Investigational | Moderate to low | Protocol discussion relies on trial methods, not an approved label |
This is why competitor articles often blur the line between published trial data and speculative user dosing. That gap is exactly where a better page wins. It stays precise about what is known, what is inferred, and what remains unsettled.
If you want the big-picture comparison, start with retatrutide vs semaglutide, tirzepatide vs semaglutide, and our broader peptides for weight loss hub. Also include a text look at the best peptide companies if sourcing quality is part of the decision.
Research sourcing and vendor options
Weight-loss cluster articles on PeptidePick use a different vendor order than recovery or skin pages. For this topic, Apollo Peptide Sciences fits the GLP-first angle. Limitless Biotech works if someone wants more delivery formats. Pinnacle Peptide Labs adds another established catalog with a standing discount code.
That said, vendor choice does not solve the evidence problem. For retatrutide, the protocol conversation still has to start with human trials, not storefront copy.
Need another source with strong peptide catalog depth?
Pinnacle Peptide Labs carries a wide range of metabolic, longevity, and recovery compounds, including GLP research categories.
99% pure research peptides - use code Peptidepick15 for 15% off
Use code Peptidepick15 for 15% off your order
Readers who want a stronger foundation before looking at vials should also review our retatrutide overview, retatrutide side effects, and are peptides legal. Those pages answer the surrounding questions that usually come up before or after dose research.
Retatrutide dosage protocol FAQ
Is there an FDA-approved retatrutide dose?
No. Retatrutide remains investigational, so there is no FDA-approved label dose at the time of writing.
How was retatrutide dosed in obesity trials?
Published trial reporting describes once-weekly dosing with gradual escalation to maintenance arms that included 1 mg, 4 mg, 8 mg, and 12 mg.
Why do people talk about titration instead of a fixed starting dose?
Because gastrointestinal side effects increase as dose rises. Titration is a tolerability tool, not just a scheduling detail.
Can retatrutide be compared directly with semaglutide or tirzepatide dosing?
Only in a limited way. Semaglutide and tirzepatide have FDA-approved products with labeled dosing, while retatrutide still relies on trial-stage evidence.
Does reconstitution change the actual protocol?
No. Reconstitution changes concentration and syringe-unit math, not the underlying protocol target in milligrams.
What is the biggest uncertainty around retatrutide dosing right now?
The open question is how future phase 3 and eventual labeling, if approved, will define the best balance between efficacy and tolerability at higher doses.
Related articles
- Retatrutide Peptide: The Triple-Receptor Agonist Redefining Weight Loss Research
- Retatrutide Side Effects: What Research Shows and How to Manage Them
- Tirzepatide Dosage Guide: Protocols, Titration, and Research Data
- Retatrutide vs Semaglutide: Comparing Weight Loss Peptides
- Best Peptides for Weight Loss: Ranked by Research Strength
- Compounded Semaglutide vs Ozempic: What Actually Changes?