Retatrutide vs Tirzepatide: How These GLP-1 Drugs Compare
Retatrutide vs tirzepatide is the comparison many weight-loss researchers are watching in 2026. Tirzepatide is already an FDA-approved dual incretin drug. Retatrutide is still investigational, but its phase 2 and phase 3 data show weight-loss numbers that are hard to ignore.
TLDR: Tirzepatide activates GIP and GLP-1 receptors and has published 72-week obesity trial data plus FDA-approved products. Retatrutide activates GIP, GLP-1, and glucagon receptors. In Lilly's 2026 TRIUMPH-1 release, the 12 mg retatrutide arm averaged 28.3% body-weight loss at 80 weeks, while the earlier NEJM phase 2 trial showed up to 24.2% at 48 weeks.
The tradeoff is maturity. Tirzepatide has the stronger approval and prescribing record. Retatrutide has the stronger early efficacy signal, but it remains legally available only through clinical trials.
Retatrutide vs Tirzepatide: Quick Comparison
The short version: tirzepatide is the proven, approved option. Retatrutide is the more experimental triple-agonist candidate.
That does not make one automatically "better." It depends on what question is being asked. A clinician treating a patient today is dealing with tirzepatide. A researcher studying the next wave of incretin pharmacology is probably watching retatrutide closely.
| Factor | Retatrutide | Tirzepatide |
|---|---|---|
| Drug class | Triple receptor agonist | Dual receptor agonist |
| Targets | GIP, GLP-1, glucagon | GIP, GLP-1 |
| Approval status | Investigational, not FDA-approved | FDA-approved in prescription products |
| Published obesity data | NEJM phase 2, 48 weeks; Lilly phase 3 topline, 80 weeks | NEJM SURMOUNT-1, 72 weeks |
| Best reported average loss | 28.3% at 80 weeks in TRIUMPH-1 topline data | Up to 20.9% at 72 weeks in SURMOUNT-1 |
For broader context on GLP-1 and related compounds, see our guide to peptides for weight loss and the ranked best peptides for weight loss comparison.
Researching GLP-1 Peptide Sourcing?
Apollo Peptide Sciences specializes in GLP-1 research peptides and growth-factor compounds for lab use.
Shop Apollo Peptide Sciences →
Specializing in GLP-1 research peptides and growth factors
Retatrutide vs Tirzepatide Mechanism
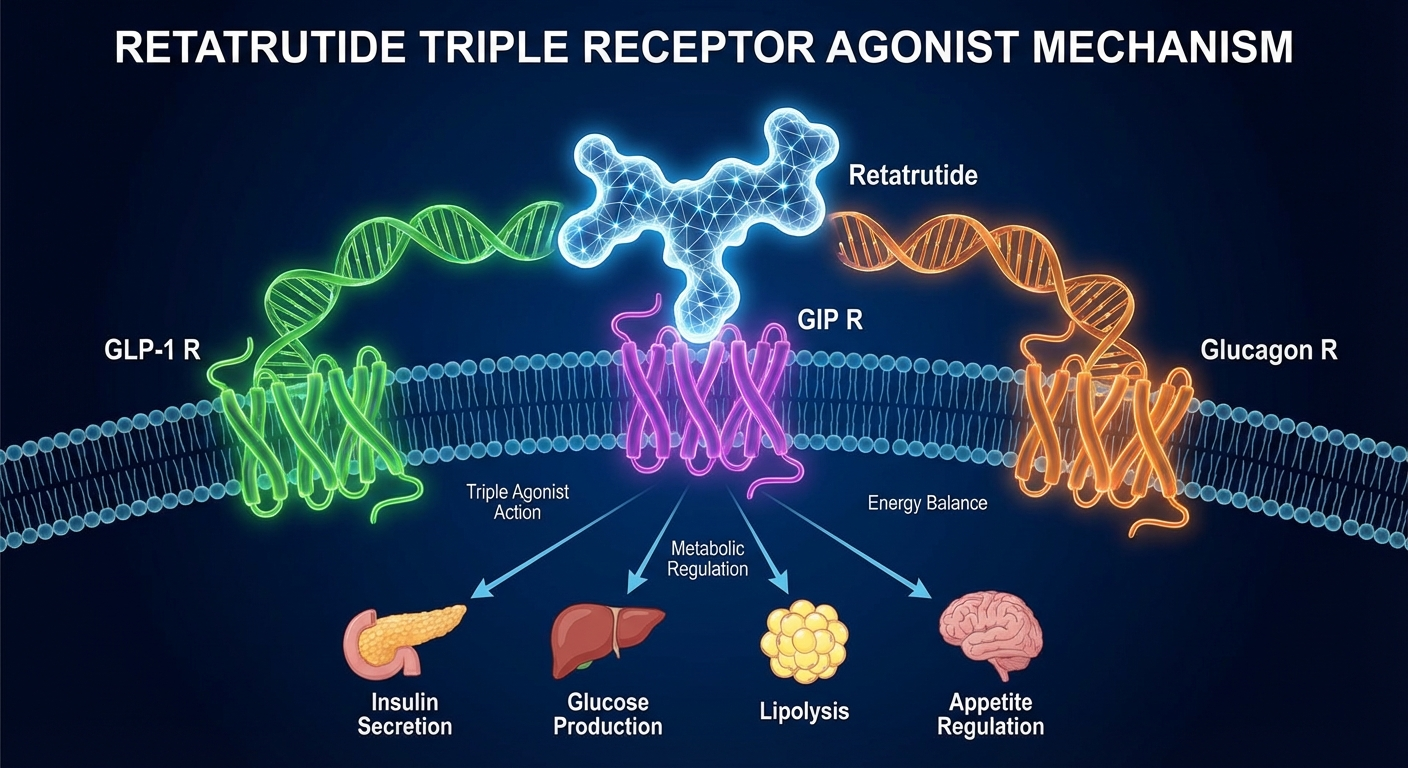
Tirzepatide works through GIP and GLP-1 receptor agonism. GLP-1 signaling is associated with appetite reduction, slower gastric emptying, and glucose-dependent insulin secretion. GIP adds another incretin pathway that may improve the weight-loss effect when paired with GLP-1.
Retatrutide adds glucagon receptor activity to that same GIP and GLP-1 backbone. That is the main scientific difference. The glucagon piece is interesting because glucagon can affect energy expenditure and liver metabolism, but it also adds uncertainty.
More receptors can mean more effect. It can also mean harder tolerability and dose tuning.
That nuance matters. Retatrutide's larger weight-loss signal may come partly from adding glucagon agonism, but phase 3 publications and FDA review will matter more than excitement around the mechanism.
Why the glucagon receptor matters
Glucagon is often discussed only as a blood-sugar hormone. In obesity drug research, it is also studied for effects on energy use and fat metabolism. Retatrutide uses that pathway as part of a triple agonist design.
But this is where the comparison stops being simple. A stronger pharmacology profile is not automatically a better real-world drug. Tolerability, lean-mass preservation, gallbladder risk, heart-rate effects, and discontinuation rates all matter.
Retatrutide vs Tirzepatide Weight-Loss Results
The headline numbers favor retatrutide. The evidence base still favors tirzepatide.
In the NEJM retatrutide phase 2 trial, adults with obesity or overweight without diabetes received once-weekly retatrutide or placebo for 48 weeks. The authors reported dose-dependent weight reduction, with the highest tested dose groups producing average losses around the mid-20% range by week 48.
Lilly's May 21, 2026 TRIUMPH-1 release moved the story forward. In that 80-week phase 3 trial, participants on 12 mg retatrutide lost an average of 70.3 pounds, or 28.3% of body weight. Lilly also reported that 45.3% of participants in that arm lost at least 30% of body weight.
Tirzepatide's main obesity benchmark is SURMOUNT-1. In the NEJM 72-week trial, adults with obesity or overweight without diabetes received 5 mg, 10 mg, or 15 mg once weekly. The 15 mg group averaged 20.9% weight reduction, compared with 3.1% for placebo.
- Retatrutide phase 2: published NEJM data over 48 weeks.
- Retatrutide TRIUMPH-1: Lilly-reported phase 3 topline data over 80 weeks, with publication still needed for full peer review.
- Tirzepatide SURMOUNT-1: peer-reviewed NEJM obesity data over 72 weeks.
- Tirzepatide diabetes data: additional trials support weight and glycemic effects in type 2 diabetes populations.
So, is retatrutide stronger than tirzepatide? Based on available obesity efficacy signals, probably. But the honest answer is narrower: retatrutide has reported higher average weight loss in its trial program, while tirzepatide has approved-label use and more mature clinical context.
For deeper single-drug background, read our retatrutide peptide guide, retatrutide dosage protocol, and tirzepatide dosage guide.
Side Effects and Safety Signals
The side-effect overlap is not surprising. Both drugs act on incretin pathways, so gastrointestinal effects show up often.
Commonly reported issues include nausea, diarrhea, vomiting, constipation, reduced appetite, and abdominal discomfort. With incretin drugs, symptoms often cluster around dose escalation. That does not make them harmless. It means trial design and titration speed matter.
Tirzepatide labeling includes boxed-warning language about thyroid C-cell tumors observed in rats, with unknown human relevance. It is contraindicated for patients with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2.
Retatrutide is still under investigation. Its safety profile cannot be treated as settled until regulators review the full package. The 2026 phase 3 topline result is important, but topline releases are not the same as full prescribing information.

There is also a body-composition question. Large weight loss can include both fat mass and lean mass. That is not unique to retatrutide or tirzepatide, but it becomes more relevant as average losses move above 20% of body weight.
Largest Delivery-Form Variety
Limitless Biotech uses a free VIP account flow that opens its full research catalog, including injectable, spray, and capsule formats for many compounds.
Create your free Limitless account first, then use code PeptidePick for a discount at checkout
118+ research peptides in injectable, spray, and capsule forms - create a free account to access the full catalog
Legal Status: Retatrutide Is Not the Same as Tirzepatide
This is the part many comparison pages blur. Retatrutide and tirzepatide are not on equal legal footing.
The FDA approved Zepbound, a tirzepatide injection, for chronic weight management in adults with obesity or overweight with at least one weight-related condition in November 2023. Tirzepatide is also the active ingredient in Mounjaro for type 2 diabetes.
Retatrutide is different. Lilly describes it as an investigational molecule. In its 2026 TRIUMPH-1 release, Lilly stated that retatrutide is legally available only to participants in Lilly clinical trials. That line matters for consumers and researchers looking at online "retatrutide" offers.
Any non-trial retatrutide product sold online should be viewed as unapproved and outside the FDA drug approval pathway. That does not mean every research-labeled vial is automatically fake, but it does mean buyers do not have the same manufacturing, labeling, or clinical oversight that applies to approved prescription medication.
The gap is practical, not just legal. Approved products have label-defined strengths, adverse-event reporting, and inspected supply chains. Research-market products can vary by seller, batch, storage history, and documentation quality.
Research Sourcing Notes for Retatrutide and Tirzepatide
For readers comparing research suppliers, the safer starting point is vendor quality control rather than hype around any one compound. The basics still matter: identity testing, purity documentation, batch-specific COAs, clear storage notes, and realistic labeling.
A vendor page that hides testing details is a weak research source, even if the price looks attractive. Batch paperwork should be easy to match against the product, not buried behind vague claims. Clear documentation will not make an investigational drug approved, but it does reduce avoidable research uncertainty.
PeptidePick keeps a separate best peptide companies guide for research-supplier comparisons. Use that before clicking a random ad with suspicious discount language.
Also use the basic lab-reference tools before handling lyophilized material. The free peptide reconstitution calculator and how to reconstitute peptides guide explain volume math, concentration, and bacteriostatic-water handling in research settings.
One more thing: oral supplement alternatives are a different category. Nootropics Depot sells third-party tested oral supplements, not injectable peptides. It can be relevant for readers comparing non-injectable wellness options, but it should not be treated as a source for retatrutide or tirzepatide research peptides.
Retatrutide vs Tirzepatide: Which Looks More Promising?
Retatrutide looks more potent on weight-loss numbers. Tirzepatide looks more dependable from a regulatory and clinical-use standpoint.
That is the real split. If the question is "which produced the largest average weight loss in available obesity data," retatrutide has the edge. If the question is "which can a physician prescribe today under an FDA-approved obesity label," tirzepatide wins.
But the final answer may change once retatrutide's full phase 3 data are published and reviewed. Topline press releases can be accurate and still incomplete. Peer-reviewed methods, subgroup data, adverse-event tables, discontinuation patterns, and label language will decide how impressive the drug really is.
Compare High-Purity Research Peptides
Pinnacle Peptide Labs carries GLP-1SG, GLP-2TZ, GLP-3RT, and related research compounds with a reader discount.
Use code Peptidepick15 for 15% off your order
99% pure research peptides - use code Peptidepick15 for 15% off
FAQ
Is retatrutide stronger than tirzepatide?
Available obesity data suggest retatrutide may produce greater average weight loss than tirzepatide. Lilly reported 28.3% average body-weight loss at 80 weeks for 12 mg retatrutide in TRIUMPH-1, while SURMOUNT-1 reported up to 20.9% at 72 weeks for 15 mg tirzepatide.
Is retatrutide FDA-approved?
No. Retatrutide is investigational as of June 11, 2026. Lilly has stated that retatrutide is legally available only to clinical-trial participants.
Is tirzepatide FDA-approved?
Yes. Tirzepatide is FDA-approved in prescription products, including Zepbound for chronic weight management and Mounjaro for type 2 diabetes.
What receptors does retatrutide target?
Retatrutide targets GIP, GLP-1, and glucagon receptors. That triple-receptor design separates it from tirzepatide, which targets GIP and GLP-1.
What are the main side effects?
The most common side effects in this drug family are gastrointestinal, including nausea, vomiting, diarrhea, constipation, and appetite reduction. Approved tirzepatide labeling also includes warnings and contraindications that should be reviewed with a licensed clinician.
Can retatrutide and tirzepatide be stacked?
No approved clinical protocol supports stacking retatrutide with tirzepatide. Combining incretin agonists could increase adverse effects and should not be treated as a casual research shortcut.
Which one is better for research comparison articles?
Retatrutide is better for studying next-generation triple agonism. Tirzepatide is better for comparing an approved dual incretin drug with a larger real-world and label history.
Related Articles
- Retatrutide vs Semaglutide
- Tirzepatide vs Semaglutide
- Retatrutide Side Effects
- Compounded Semaglutide vs Ozempic
- Natural Ozempic Alternatives
- Semaglutide Guide
Sources
- Jastreboff AM et al. "Triple-Hormone-Receptor Agonist Retatrutide for Obesity - A Phase 2 Trial." New England Journal of Medicine, 2023.
- Jastreboff AM et al. "Tirzepatide Once Weekly for the Treatment of Obesity." New England Journal of Medicine, 2022.
- Garvey WT et al. "Tirzepatide once weekly for the treatment of obesity in people with type 2 diabetes." The Lancet, 2023.
- U.S. FDA. "FDA Approves New Medication for Chronic Weight Management." November 8, 2023.
- Eli Lilly. "Lilly's triple agonist, retatrutide, delivered powerful weight loss in pivotal Phase 3 obesity trial." May 21, 2026.