FDA research disclaimer: Peptides discussed on PeptidePick may be sold for laboratory research only. They are not intended to diagnose, treat, cure, or prevent any disease. This guide is educational and is not medical advice. Talk with a licensed clinician before using any injectable medication or research compound.
Where to Inject Peptides: Site Selection and Rotation Guide
TLDR: Where to inject peptides usually depends on the route listed in the protocol, the compound, and clinician guidance. For subcutaneous protocols, common sites include the abdomen away from the navel, outer thigh, upper outer buttock, and back of the upper arm.
The safer pattern is simple: use clean technique, choose fatty tissue, rotate sites, avoid irritated skin, and track where each injection happened. That is boring advice. It is also the advice that prevents most avoidable site problems.
People search where to inject peptides because the vial, syringe, and dose math only answer part of the question. The site matters too. A bad site can hurt more, absorb less predictably, or turn into a sore lump that makes the next injection harder.
This guide focuses on research and education. It pulls from subcutaneous injection guidance, injection safety literature, FDA warnings on compounded GLP-1 dosing errors, and practical site-rotation logic used in peptide research settings.
Best Places Where to Inject Peptides Subcutaneously
Most research peptide protocols that involve self-administration use the subcutaneous route, often shortened to SubQ. That means the injection goes into the fatty layer below the skin, not deep into muscle.
Johns Hopkins Arthritis Center describes common subcutaneous areas as the outer upper arm, top of the thigh, buttocks, and abdomen except around the navel or waistline. That same site logic is used across many self-injection instructions because those areas usually have pinchable tissue.
| Site | Typical use case | Watch for |
|---|---|---|
| Abdomen | Common SubQ site with easy access and usually enough fatty tissue. | Stay at least a couple inches away from the navel and avoid waistbands. |
| Outer thigh | Useful when abdomen sites need a break. | Avoid injecting into firm muscle or areas rubbed by tight clothing. |
| Upper outer buttock | Often has enough subcutaneous tissue for rotation. | Harder to see and clean well without help. |
| Back of upper arm | Common in clinical teaching materials. | Difficult for solo injections unless mobility is good. |
For peptide-specific setup work, pair this site guide with the free peptide reconstitution calculator and the how to reconstitute peptides guide. Site choice does not fix bad concentration math.
Researching GLP-1 Peptide Protocols?
Apollo Peptide Sciences carries GLP-1 research peptides plus bacteriostatic water for lab protocols that require careful preparation.
Shop Apollo Peptide Sciences →
Specializing in GLP-1 research peptides and growth factors
Where Not to Inject Peptides
The short answer: do not inject into angry skin. Avoid bruises, scars, moles, rashes, hard lumps, open wounds, stretch marks that feel tender, and any area that looks infected.
Also avoid spots that will be compressed after the injection. A waistband, tight gym shorts, or a chair edge can turn a clean site into a sore one. The goal is not just to get the needle in. The goal is to leave the tissue alone afterward.
There is nuance here. Some peptides are discussed online as if any fatty spot is fine. That is too casual. Injection site choice should match the compound's intended route, the syringe size, the volume, and medical guidance.
For needle sizing context, see the best gauge needle for peptide injections guide. If the protocol is intramuscular, this article is not enough on its own. Read the SubQ vs intramuscular injection for peptides guide before comparing routes.
Where to Inject Peptides When Rotating Sites
Rotation means moving injections around in a pattern so the same small patch of tissue is not hit again and again. This matters because repeated injections in one area can irritate tissue and may cause lumps or thickened spots.
Injection-technique research in insulin users is useful here because insulin is also commonly given subcutaneously. Reviews in Clinical Diabetes and related diabetes literature describe poor rotation as a frequent factor tied to lipohypertrophy, which means fatty thickening under the skin.
Peptide users should not overread insulin data as peptide-specific proof. But the tissue lesson transfers: repeated needle trauma in the same spot is a bad habit.
- Move at least one finger-width away from the last site within the same region.
- Use the left and right sides of the body instead of favoring one side.
- Track sites in a note, spreadsheet, or printed chart.
- Pause any area that feels lumpy, painful, warm, or unusually firm.
A practical pattern is abdomen left, abdomen right, thigh left, thigh right, then repeat only if the tissue feels normal. Some researchers prefer to stay within one region for consistency, then rotate within that region. That can make sense when absorption consistency matters.
But if the same abdomen quadrant gets used every time, it is not real rotation. It is just habit with a different label.
Need More Delivery-Form Options?
Limitless Biotech lists a wide catalog with injectable, spray, and capsule formats after free account registration.
118+ research peptides in injectable, spray, and capsule forms - create a free account to view the full catalog
Use code PeptidePick for a discount at checkout after joining the VIP account
SubQ vs IM: Where to Inject Peptides Depends on the Route
Subcutaneous and intramuscular injections are not interchangeable. SubQ aims for fatty tissue. IM aims for muscle. The same needle length, angle, and site plan may not fit both routes.
Many peptide discussions online blur that line, especially with compounds such as BPC-157, TB-500, CJC-1295, ipamorelin, or GLP-1 research peptides. A protocol that says SubQ should not be casually changed to IM because someone on a forum preferred a different site.
For GLP-1 medications, FDA-approved products are designed around specific instructions and devices. The FDA has also warned about dosing errors with compounded injectable semaglutide products, including cases where people measured five to twenty times the intended amount. That warning is about dosing, but it points to the same problem: injection setup mistakes can become real medical events.
If the issue is dose math, start with the peptide dosage calculator and how to measure peptides in mcg. If the issue is the compound itself, read the relevant peptide guide first. For example, GLP-1 readers may want the tirzepatide dosage guide or microdosing semaglutide.
Safety Checks Before Choosing Where to Inject Peptides
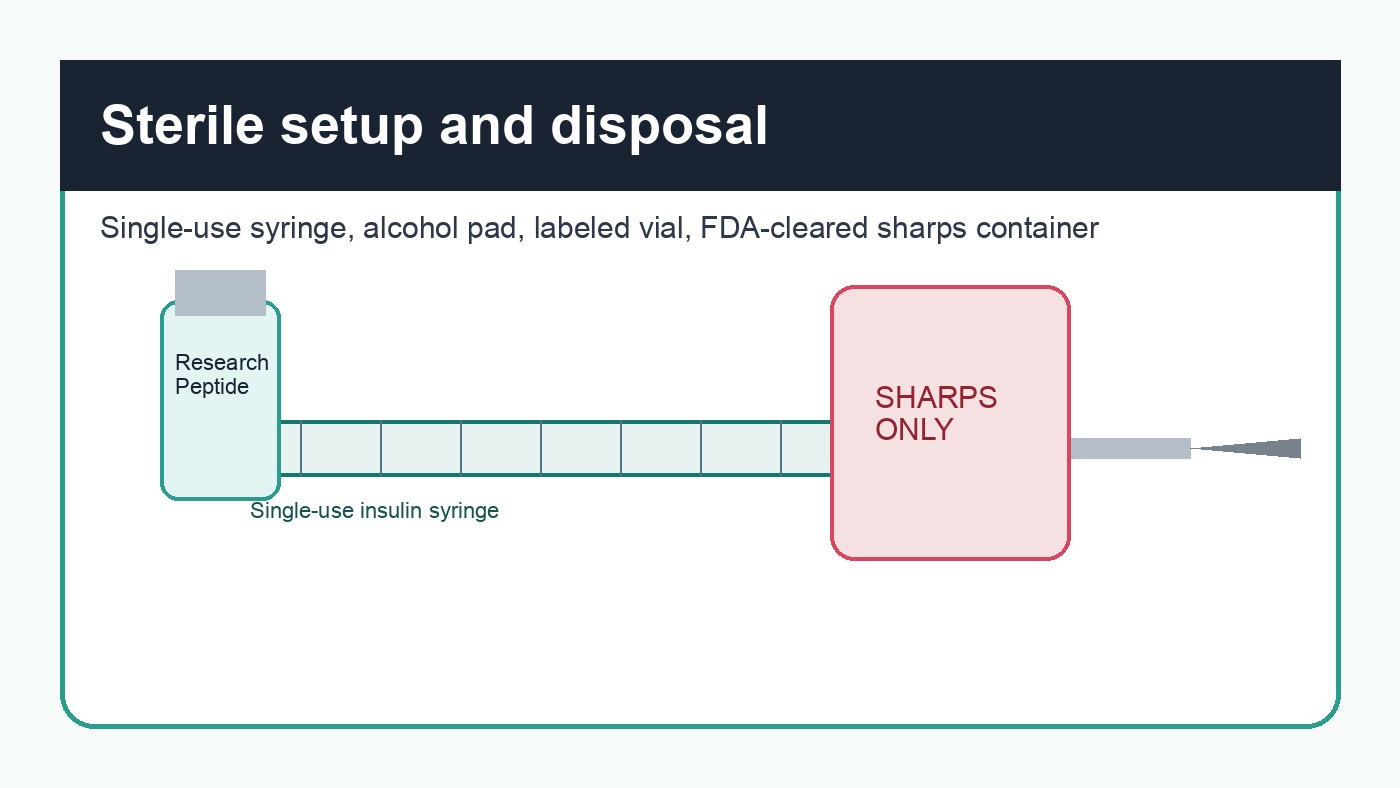
The CDC's safe injection guidance is blunt: use a sterile, single-use needle and syringe for each injection, prevent contamination, and discard used injection equipment properly. That guidance is written for health care settings, but the principle is not optional for self-injection education.
Before any injection, the basic checks are simple. The peptide should be identified, the concentration should be known, the syringe units should match the calculation, and the site should be clean. The vial should not be cloudy, discolored, or full of unexpected particles unless that appearance is expected for the product.
There is one point worth being strict about: never use an injection site to compensate for uncertainty. If the dose, concentration, sterility, or route is unclear, the right move is to stop and verify. Picking a different body part does not solve a preparation problem.
- Use a new sterile syringe and needle each time.
- Wash hands and clean the vial stopper before drawing.
- Clean the skin and let it dry before the injection.
- Dispose of sharps in a proper sharps container.
- Seek medical help for spreading redness, fever, severe pain, or signs of allergic reaction.
Readers comparing vendors should use the best peptide companies guide as a body text reference, not as a shortcut around safety. Vendor quality matters. Technique still matters.
Common Mistakes With Peptide Injection Sites
The most common mistake is treating the abdomen as one site. It is not. The abdomen is a region with many possible spots, and repeated injections in the same two-inch area defeat the whole point of rotation.
Another mistake is injecting into tissue that already feels different. Lumps, dents, thickened patches, and unusual tenderness are feedback. Ignore that feedback and the rotation plan becomes cosmetic.
People also underestimate clothing. A technically good thigh injection can still get irritated if tight fabric rubs it for the next six hours. So site choice should account for the rest of the day, not just the injection moment.
Research Notes Behind This Guide
The strongest site-selection evidence comes from established injection teaching and insulin literature, not from controlled trials of every individual research peptide. That is a limitation. It would be cleaner if every peptide had route-specific site studies, but most do not.
Still, the source pattern is consistent. Johns Hopkins lists the abdomen, thigh, buttock, and upper arm as common SubQ sites. CDC injection safety materials stress sterile single-use equipment. FDA warnings on compounded GLP-1 products show how self-injection errors can lead to serious outcomes when dose measurement and preparation are unclear.
For injection-site reactions tied to specific GLP-1 research, PeptidePick has a deeper guide on tirzepatide injection site reaction. For broader rotation planning, see peptide injection site rotation.
Prefer a Discount-Driven Peptide Vendor?
Pinnacle Peptide Labs carries common research peptides, GLP-1 options, and recovery stacks for researchers comparing catalog depth and price.
99% pure research peptides - use code Peptidepick15 for 15% off
Use code Peptidepick15 for 15% off your order
Ascension Peptides is another approved PeptidePick vendor with 60+ third-party tested research peptides and stacks. It is a better fit for some recovery and cognitive peptide topics, while this article's main CTAs focus on GLP-1, delivery-form variety, and discount access.
For readers who do not want injectable research products at all, Nootropics Depot is an oral supplement alternative for categories such as amino acids, mushroom extracts, adaptogens, and nootropics. It is not an injectable peptide vendor.
Related Articles
- Peptide Injection Site Rotation
- Best Gauge Needle for Peptide Injections
- SubQ vs Intramuscular Injection for Peptides
- Bacteriostatic Water for Injection
- How to Store Peptides
- Best Peptide Companies
FAQ: Where to Inject Peptides
Where is the best place to inject peptides?
For many SubQ peptide protocols, common sites include the abdomen away from the navel, outer thigh, upper outer buttock, and back of the upper arm. The best site depends on the prescribed or research route, the volume, and whether the tissue is healthy.
Can peptides be injected into the stomach?
Many subcutaneous protocols use the abdomen because it usually has accessible fatty tissue. Avoid the navel area, scars, bruises, irritated skin, and any spot that feels lumpy or painful.
Should peptide injection sites be rotated?
Yes. Rotation reduces repeated trauma to the same tissue. Insulin injection research links poor rotation with lipohypertrophy, and the same tissue-care logic is useful for peptide site planning.
Can peptides be injected into muscle?
Only if the protocol or clinician specifically calls for intramuscular administration. SubQ and IM routes use different target tissue, site logic, and often different needle length.
What happens if a peptide injection site gets red or swollen?
Mild short-lived irritation can happen with injections, but spreading redness, warmth, severe pain, pus, fever, or allergic symptoms need medical attention. Do not keep using an irritated site.
How far apart should injection sites be?
A practical minimum is at least one finger-width away from the last injection within the same region, with broader rotation across left and right sides. If tissue feels abnormal, give that area a longer break.
Affiliate disclosure: PeptidePick may earn a commission when readers buy through approved affiliate links in this article. This does not change the price you pay or our research standards.